A single drug can shrink or cure human breast, ovary, colon, bladder, brain, liver, and prostate tumors that have been transplanted into mice, researchers have found. The treatment, an antibody that blocks a "do not eat" signal normally displayed on tumor cells, coaxes the immune system to destroy the cancer cells.
A decade ago, biologist Irving Weissman of the Stanford University School of Medicine in Palo Alto, California, discovered that leukemia cells produce higher levels of a protein called CD47 than do healthy cells. CD47, he and other scientists found, is also displayed on healthy blood cells; it's a marker that blocks the immune system from destroying them as they circulate. Cancers take advantage of this flag to trick the immune system into ignoring them. In the past few years, Weissman's lab showed that blocking CD47 with an antibody cured some cases of lymphomas and leukemias in mice by stimulating the immune system to recognize the cancer cells as invaders. Now, he and colleagues have shown that the CD47-blocking antibody may have a far wider impact than just blood cancers.
"What we've shown is that CD47 isn't just important on leukemias and lymphomas," says Weissman. "It's on every single human primary tumor that we tested." Moreover, Weissman's lab found that cancer cells always had higher levels of CD47 than did healthy cells. How much CD47 a tumor made could predict the survival odds of a patient.
To determine whether blocking CD47 was beneficial, the scientists exposed tumor cells to macrophages, a type of immune cell, and anti-CD47 molecules in petri dishes. Without the drug, the macrophages ignored the cancerous cells. But when the anti-CD47 was present, the macrophages engulfed and destroyed cancer cells from all tumor types.
Next, the team transplanted human tumors into the feet of mice, where tumors can be easily monitored. When they treated the rodents with anti-CD47, the tumors shrank and did not spread to the rest of the body. In mice given human bladder cancer tumors, for example, 10 of 10 untreated mice had cancer that spread to their lymph nodes. Only one of 10 mice treated with anti-CD47 had a lymph node with signs of cancer. Moreover, the implanted tumor often got smaller after treatment—colon cancers transplanted into the mice shrank to less than one-third of their original size, on average. And in five mice with breast cancer tumors,
anti-CD47 eliminated all signs of the cancer cells, and the animals remained cancer-free 4 months after the treatment stopped.
"We showed that even after the tumor has taken hold, the antibody can either cure the tumor or slow its growth and prevent metastasis," says Weissman.
Although macrophages also attacked blood cells expressing CD47 when mice were given the antibody, the researchers found that the decrease in blood cells was short-lived; the animals turned up production of new blood cells to replace those they lost from the treatment, the team reports online today in the Proceedings of the National Academy of Sciences.
Cancer researcher Tyler Jacks of the Massachusetts Institute of Technology in Cambridge says that although the new study is promising, more research is needed to see whether the results hold true in humans. "The microenvironment of a real tumor is quite a bit more complicated than the microenvironment of a transplanted tumor," he notes, "and it's possible that a real tumor has additional immune suppressing effects."
Another important question, Jacks says, is how CD47 antibodies would complement existing treatments. "In what ways might they work together and in what ways might they be antagonistic?" Using anti-CD47 in addition to chemotherapy, for example, could be counterproductive if the stress from chemotherapy causes normal cells to produce more CD47 than usual.
Weissman's team has received a $20 million grant from the California Institute for Regenerative Medicine to move the findings from mouse studies to human safety tests. "We have enough data already," says Weissman, "that I can say I'm confident that this will move to phase I human trials."
*Correction, 2 April 2013: One reference to the compound used to treat mice was previously named as CD47, but in all cases was the antibody to that protein, anti-CD47.




![[Source: Broad Institute]](http://singularityhub.com/wp-content/uploads/2013/05/image2A6.jpg)
![Nano-networks of porous beads are engineered to respond to high levels of blood sugar by releasing insulin. [Source: Journal of Agriculture and Food Chemistry]](http://singularityhub.com/wp-content/uploads/2013/05/nano.jpg)


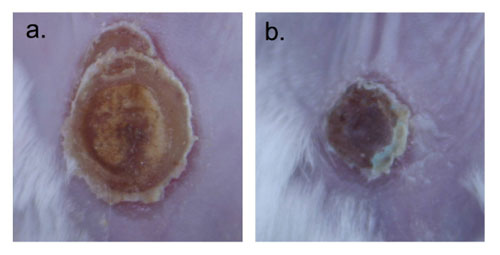 Images were taken on day 9 after infection. a) is topically applied solubilized Amphotericin B and b) Amphotericin B nanoparticle applied. (Images: Dr. Friedman, Montefiore - Albert Einstein College of Medicine)Materials at the nanoscale have a greater likelihood of interacting with their desired target, here, the cell wall, and therefore the payloads have greater efficacy. Furthermore, the nanoparticles themselves can physically damage pathogen structures and prevent cell-to-cell communication and sharing of resources, offering synergists but different antifungal properties.Encapsulating amphotericin in nanoparticles not only made it more effective, but also allowed for it to be directly and topically applied to a wound – an option not currently available. Systemic delivery, while very effective, comes at a great cost as amphotericin has multiple well established side effects and toxicities associated with its use.Our team here at Einstein represents a broad range of expertise calling from multiple departments including medicine (infectious diseases, dermatology), physiology and biophysics, and immunology and microbiology, highlighting the multidisciplinary nature of nanotechnology research. Other authors included David Sanchez; David Schairer; Chaim Tuckman-Vernon; Jason Chouake; Allison Kutner; Joy Makdisi; Joel Friedman; and Joshua d Nosanchuk.By Dr. Adam Friedman, Assistant Professor of Medicine (Dermatology)/ Physiology and Biophysics, and Director of Dermatologic Research at Montefiore Medical Center - Albert Einstein College of Medicine.
Images were taken on day 9 after infection. a) is topically applied solubilized Amphotericin B and b) Amphotericin B nanoparticle applied. (Images: Dr. Friedman, Montefiore - Albert Einstein College of Medicine)Materials at the nanoscale have a greater likelihood of interacting with their desired target, here, the cell wall, and therefore the payloads have greater efficacy. Furthermore, the nanoparticles themselves can physically damage pathogen structures and prevent cell-to-cell communication and sharing of resources, offering synergists but different antifungal properties.Encapsulating amphotericin in nanoparticles not only made it more effective, but also allowed for it to be directly and topically applied to a wound – an option not currently available. Systemic delivery, while very effective, comes at a great cost as amphotericin has multiple well established side effects and toxicities associated with its use.Our team here at Einstein represents a broad range of expertise calling from multiple departments including medicine (infectious diseases, dermatology), physiology and biophysics, and immunology and microbiology, highlighting the multidisciplinary nature of nanotechnology research. Other authors included David Sanchez; David Schairer; Chaim Tuckman-Vernon; Jason Chouake; Allison Kutner; Joy Makdisi; Joel Friedman; and Joshua d Nosanchuk.By Dr. Adam Friedman, Assistant Professor of Medicine (Dermatology)/ Physiology and Biophysics, and Director of Dermatologic Research at Montefiore Medical Center - Albert Einstein College of Medicine.
